Vagus nerve stimulation has a legitimate, decades-long clinical history — but most of that history is in implanted devices for specific medical conditions, not the consumer wearables marketed today for everyday stress and anxiety. Here's where the evidence actually sits, and what distinction matters most when evaluating any device in this category.

Vagus Nerve Stimulation for Anxiety: Two Very Different Categories of Evidence
When evaluating claims about VNS and anxiety, the most important distinction is between implanted (invasive) VNS and transcutaneous (non-invasive, taVNS) approaches — because their evidence bases are not interchangeable, and marketing in this category frequently implies they are.
Implanted VNS has been used clinically since the 1990s, primarily for treatment-resistant epilepsy, and was subsequently approved in some markets for treatment-resistant depression. This is a surgical procedure involving a device implanted near the chest wall with a lead running to the vagus nerve in the neck. The evidence base here spans decades and thousands of patients, for those specific conditions.
Consumer taVNS devices — ear-clip devices, wrist wearables, and similar — are categorically different. They deliver mild electrical stimulation through the skin to vagal nerve branches accessible at the outer ear or elsewhere on the body. The mechanism is plausible, but the clinical evidence base, particularly for everyday anxiety and stress in healthy adults, is considerably smaller and more recent.
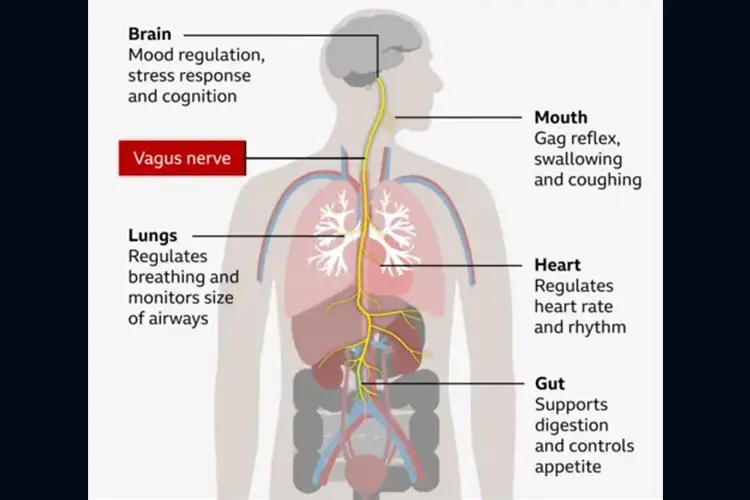
Understanding this distinction is covered in more detail in our full guide to the vagus nerve and how it works.
What taVNS Anxiety Research Actually Shows So Far
A number of smaller studies and early-stage trials report reductions in self-reported anxiety measures and changes in physiological markers like HRV following taVNS sessions. A 2024 randomised controlled trial published in Frontiers in Integrative Neuroscience found significant reductions in anxiety scores in university students with elevated anxiety following active taVNS compared to sham stimulation, with 42 participants across groups.
This is encouraging, but it's also a small trial, in a specific population, over a short duration. That pattern — promising but limited — is characteristic of the broader taVNS-anxiety literature at this stage. Larger, longer, placebo-controlled trials specifically in everyday anxiety populations (rather than clinical, perioperative, or depressive-disorder populations) are still limited.
There is also a critical distinction worth internalising: many studies in this category measure physiological markers like HRV as their primary outcome, not anxiety symptom scores. A study showing that taVNS increases HRV has not necessarily demonstrated a reduction in felt anxiety. Those are related but different outcomes, and marketing that treats a physiological marker as proof of symptom relief is conflating them.
HRV as an Outcome: What It Does and Doesn't Tell You
HRV is a widely used proxy for vagal tone — a higher HRV indicates greater parasympathetic flexibility, which is associated with better stress resilience. It's a legitimate and useful measurement. But it's a proxy, not a direct measurement of how anxious someone feels, how well they sleep, or how they function under stress.
A device that reliably increases HRV during sessions is doing something measurable and physiologically meaningful. Whether that consistently produces a felt reduction in anxiety, improved sleep, or better cognitive performance is a separate question that requires separate, longer-term studies with validated symptom measures — not just HRV data.
What This Means Practically: Who Should and Shouldn't Rely on taVNS
If you have a diagnosed anxiety disorder and are receiving — or eligible for — professional treatment, a consumer taVNS device should be considered a possible complement to that treatment, not a replacement. It's not established as a clinical intervention for anxiety, and the evidence does not support treating it as one.
If you are dealing with everyday, sub-clinical stress — the kind that is common, exhausting, and not a psychiatric diagnosis — taVNS is a biologically plausible, low-risk tool with growing supporting evidence. The honest framing is that it's a promising intervention still catching up to its marketing, not a proven anxiety treatment. For a full evidence-level comparison between Nurosym and Sensate, two of the most popular devices in this space, see our Nurosym vs Sensate comparison.
Frequently Asked Questions
Not as a primary, standalone anxiety treatment in most markets. Some VNS approaches have regulatory approvals for epilepsy and treatment-resistant depression — different indications from general consumer anxiety claims.
No. Implanted VNS for epilepsy has decades of clinical evidence for those specific conditions. Consumer taVNS stimulates the skin near vagal branches and has a considerably smaller evidence base, especially for everyday anxiety and stress.
No — never without medical guidance. Consumer taVNS devices are not established replacements for prescribed anxiety treatment. If you're considering taVNS alongside medication, discuss this with your prescribing doctor.
HRV is a physiological proxy for vagal tone, not a direct measure of anxiety symptoms. A study showing improved HRV after taVNS has not necessarily shown reduced felt anxiety — those are different outcomes, and marketing that conflates them deserves scrutiny.
LessStress.ie
LessStress.ie covers neuro-tech devices, sleep science and brain health for an Irish audience, with every product claim checked against the real peer-reviewed evidence before it gets a recommendation.
Related Articles


Sources & Further Reading
- Ferreira, L.M.A., Brites, R., Fraião, G., et al. (2024). Transcutaneous auricular vagus nerve stimulation modulates masseter muscle activity, pain perception, and anxiety levels in university students: a double-blind, randomized, controlled clinical trial. Frontiers in Integrative Neuroscience, 18. View on PMC ↗
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. (1996). Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation, 93(5), 1043–1065. View on PubMed ↗